DS vs. RNY: 10 years later
Conclusions: RYGB and GB surgeries lead to substantial weight loss in individuals with morbid obesity. However, significant weight regain occurs over the long term, and according to the only well-designed prospective controlled study, the improvement in comorbidities associated with weight loss mitigates in the long term on weight regain. There is some evidence from a retrospective study that RYGB surgery is associated with a modest decrease in long-term mortality. These results remain to be substantiated by well-designed, long-term, randomized and prospective controlled studies. The mechanisms that lead to weight regain need to be further examined and may include increase in energy intake due to enlargement of stoma and adaptive changes in the levels of gut and adipocyte hormones such as ghrelin and leptin, which regulate energy intake; decrease in physical activity; changes in energy expenditure; and other factors. In addition to weight regain, RYGB surgery is associated with frequent incidence of iron, vitamin B12, folate, calcium, and vitamin D deficiency, which requires regular supplementation and monitoring.
*****
Sugerman et al. (12) examined the database of patients who underwent RYGB surgery and reported a decrease in percent excess body weight loss from 66% at 1 yr (91% follow-up) to 52% at 10–12 yr (37% follow-up).
*****
In conclusion, RYGB and GB surgeries lead to substantial weight loss, but weight regain over the long term is not insignificant. According to the only well-designed, prospective, controlled study, the improvement in comorbidities seen initially mitigates in the long term possibly because of weight regain.
********************************
This reference doesn't come from a DS surgeon -- it talks only about banding and RNY. Take a look at the nutritional downsides section too, especially long term. Long term, the average RNY has only maintained a weight loss of about 50% of their excess weight -- that is the threshold of no longer being considered successful, and that standard is pretty damned low -- "success" being defined as having lost 50% of one's excess weight. Gee, swell, that would have me at 225 lbs frm 290. Not good enough.
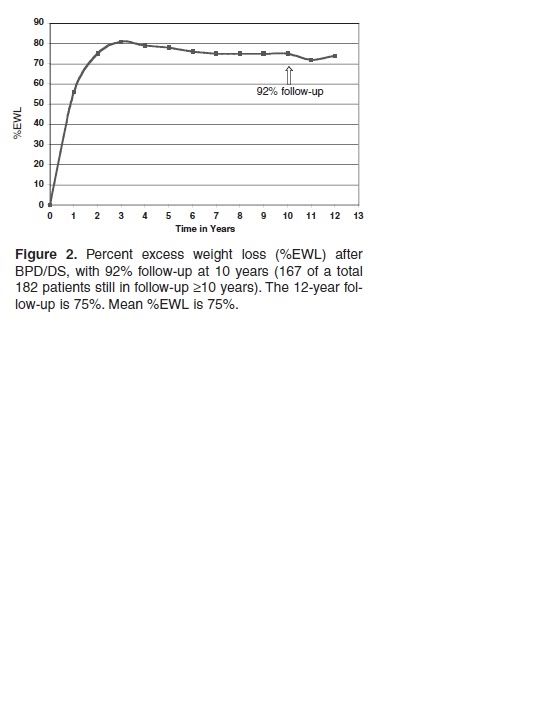
The DS long-term results are ~75% average EWL after 10 years, with 94% success rate! Hess et al., Obesity Surgery, 15, 408-416 2005.
In contrast, in Ann Surg. 2006 Nov;244(5):734-40, "Weight gain after short- and long-limb gastric bypass in patients followed for longer than 10 years," Christou NV, Look D, Maclean LD discuss the results from their practice:
OBJECTIVE: To complete a long-term (>10 years) follow-up of patients undergoing isolated roux-en-Y gastric bypass for severe obesity. BACKGROUND: Long-term results of gastric bypass in patients followed for longer than 10 years is not reported in the literature. METHODS: Accurate weights were recorded on 228 of 272 (83.8%) of patients at a mean of 11.4 years (range, 4.7-14.9 years) after surgery. Results were documented on an individual basis for both long- and short-limb gastric bypass and compared with results at the nadir BMI and % excess weight loss (%EWL) at 5 years and >10 years post surgery. RESULTS: There was a significant (P < 0.0001) increase in BMI in both morbidly obese (BMI < 50 kg/m) and super obese patients (BMI > 50 kg/m) from the nadir to 5 years and from 5 to 10 years. The super obese lost more rapidly from time zero and gained more rapidly after reaching the lowest weight at approximately 2 years than the morbidly obese patients. There was no difference in results between the long- and short-limb operations. There was a significant increase in failures and decrease in excellent results at 10 years when compared with 5 years. The failure rate when all patients are followed for at least 10 years was 20.4% for morbidly obese patients and 34.9% for super obese patients. CONCLUSIONS: The gastric bypass limb length does not impact long-term weight loss. Significant weight gain occurs continuously in patients after reaching the nadir weight following gastric bypass. Despite this weight gain, the long-term mortality remains low at 3.1%.
*********************************
In both studies, "failure" is defined as less than 50% EWL (the ASBS standard).
So, there is a 6% failure rate after 10 years for DSers, which number includes a disproporationate number of SMOs because of insurance limitations over the time period, vs. somewhere between 20% - 35% failure rate for RNYers, including those with long-limb RNY. This is a no-brainer, don't you think?
As for a direct comparison, see these charts, and you be the judge:
Even if the curves are oppositely oriented, and one measures percent weight change, and the other percent excess weight lost, and even if you assume that both DSers and RNYers end up at the same initial maximum EWL% (which isn't the case), the curves are pretty directly comparable. The first is from the Shah study; the second is from the Hess study.
Shah:

FIG. 1. Weight changes among subjects participating in the Swedish Obese Subjects study over a 10-yr period (11 ). There were 627 control subjects who did not undergo bariatric surgery, 156 who underwent banding, 451 who underwent vertical banded gastroplasty, and 34 who had gastric bypass.
Hess:


 SW 308/CW164/ GW 140
SW 308/CW164/ GW 140






 I frequently read about RNYers getting revised to... what???... yep, another RNY!
I frequently read about RNYers getting revised to... what???... yep, another RNY!