
Dangers of Vitamin Deficiencies From a Registered Dietitian’s Experience
July 28, 2016“Do I really have to take my vitamin supplements for life?” This is a very common pre-op patient question, and one that is extremely important… Because the answer is a resounding “Yes!” The dangers of vitamin deficiencies are no laughing matter, and can have lingering ramifications even if the deficiency is addressed. If left undiagnosed and untreated, the resulting adverse health consequences can lead to diminished quality of life and, in severe cases, even death.
Vitamin and Mineral Deficiencies
Post-operatively, it is more common to have multiple vitamin deficiencies than just a single deficiency (Aills et al, 2008). As the symptoms of many vitamin/mineral deficiencies are non-specific (that is, the symptoms are common symptoms such as fever, fatigue, nausea, etc.), early diagnosis is difficult without confirmation via lab work. That is yet another reason why regular follow-up with your surgeon’s office is so important. Without baseline markers against which to analyze your current lab work, your doctor may not be able to verify if there are post-operative complications, other complications due to pre-existing deficiencies, or newly onset deficiencies.
Vitamins and minerals are not just important for avoiding deficiencies; they actually work in a variety of essential ways in your body, such as nutrient absorption, energy storage and breakdown, appetite and hunger, thyroid and adrenal function, neural activities and many more (Aills et al, 2008).
Optimal intake of your supplements can help optimize your weight loss and weight maintenance long term.
Vitamins, Minerals, Food Sources, and Deficiency Symptoms
Thiamin (vitamin B1) is a water-soluble vitamin that functions as a cofactor for many enzymes, specifically involved in neurological function and carbohydrate metabolism (Frank 2011). Thiamin deficiency is known as beriberi, with “wet” beriberi manifesting with cardiac changes and edema, while “dry” beriberi manifests with muscle weakness, pain and even paralysis (Frank 2011). In more severe cases, thiamin deficiency can lead to Wernicke’s Korsakoff or Wernicke’s encephalopathy, which includes neurological impairment that can become permanent (Aills et al, 2008). Persistent vomiting can lead to thiamin deficiency, so be sure to follow up with your surgeon (Aills et al, 2008). Good sources of thiamin include meat (specifically pork), vegetables, sunflower seeds and grains (Aills et al, 2008).
Pyridoxine (vitamin B6) is a water-soluble vitamin that functions as a cofactor for more than 100 enzymes involved in amino acid metabolism and is involved in the synthesis of many other essential components such as heme (transports iron), lipids, vitamin conversion and more (Aills et al, 2008). Symptoms of deficiency include depression, confusion, swollen tongue, and neuropathy (Aills et al, 2008). Common food sources include meat, nuts, wheat bran and legumes, but it is most bioavailable in meat (Aills et al, 2008).
Cobalamin (vitamin B12) and folate (folic acid) are water-soluble vitamins that go hand in hand, as deficiency in both can lead to decreased, enlarged red blood cells (macrocytic anemia) that lack the ability to carry oxygen throughout the body (Aills et al, 2008). Pale skin, fatigue, shortness of breath, ringing in the ears, heart palpitations or rapid pulse, sore tongue, and diarrhea are just some of the symptoms of vitamin B12 deficiency (Aills et al, 2008). Continued Vitamin B
Continued Vitamin B12 deficiency can lead to pernicious anemia, characterized by peripheral nerve degeneration, pins and needles sensation, and neurological impairment, sometimes psychosis (Aills et al, 2008). Vitamin B12 is found in animal products (meat, dairy and eggs), so those consuming a vegetarian or vegan diet must be sure to supplement. Along with vitamin B12, folate is important in the maturation of red blood cells in order to transport oxygen throughout the body (Aills et al, 2008). Decreased folic acid prior to pregnancy can lead to increased risk of neural tube defects in the fetus (Aills et al, 2008). Symptoms of folate deficiency include diarrhea, swollen tongue, and cracks in one/both corners of the mouth (Aills et al, 2008). Leafy green vegetables are rich in folate, along with fruit and enriched grains (Aills et al, 2008).
Iron is an important mineral for the formation of hemoglobin and myoglobin, which help deliver oxygen from the lungs to the tissues throughout the body (Aills et al, 2008). Symptoms of deficiency can include fatigue, heart palpitations or rapid heart rate, impaired mental capacity, and difficulty swallowing (Aills et al, 2008). Iron is commonly found in meat, fish, poultry, and eggs, as well as dried fruit, enriched grains, and some vegetables and legumes (Aills et al, 2008).
Calcium is a mineral that plays an important role in bone formation, including teeth, as well as blood coagulation, and muscle contraction, including heart contractions (Aills et al, 2008). Deficiency is characterized by leg cramps, stiffness, and weakened bone strength (osteoporosis) (Aills et al, 2008). Food sources include dairy products, leafy green vegetables, legumes, and fortified foods (Aills et al, 2008).
Vitamin D, like calcium, plays an important role in bone health and helps with the absorption of calcium and phosphorus (Aills et al, 2008). Symptoms of deficiency can include softening of the bones and rachitic tetany (painful muscular spasms and tremors secondary to both calcium and vitamin D deficiency) (Aills et al, 2008). Vitamin D is a fat-soluble vitamin found in fortified dairy products, as well as eggs, fortified cereals and fatty fish such as salmon (Aills et al, 2008).
Vitamin A, a fat-soluble vitamin, helps with eye function, gene expression, reproduction function and immune function (Aills et al, 2008). Early deficiency is marked by poor wound healing, cataracts, and dry skin, while advanced deficiency can be characterized by loss of taste, extremely dry skin, corneal damage, drying of the corneas, and even blindness (Aills et al, 2008). Good sources of vitamin A include liver, fish, dairy products, and dark fruits and vegetables (Aills et al, 2008).
Vitamin E is a fat-soluble vitamin that works as an antioxidant, protecting the body’s cells from oxidative stress and free radicals (Aills et al, 2008). Deficiency of vitamin E can be characterized by muscle weakness, poor reflexes, paralysis of eye muscles, and neurologic damage (Aills et al, 2008). Vitamin E can be found in vegetable oils, grains, nuts, meats, fruits and vegetables (Aills et al, 2008).
Vitamin K is an important fat-soluble vitamin used for bone formation and blood coagulation (Aills et al, 2008). A deficiency of vitamin K can lead to easy bruising, bleeding gums, nose bleeds, heavy menstrual bleeding, and delayed blood clotting which can lead to hemorrhaging after injury (Aills et al, 2008). Vitamin K is found in green vegetables such as Brussels sprouts and cabbage, as well as vegetable oils and margarine (Aills et al, 2008)
Zinc is a mineral important to enzymes, protein synthesis, gene expression, wound healing, skin integrity, reproduction and growth (Aills et al, 2008). Symptoms of deficiency can include decreased taste sensation, altered sense of smell, decreased appetite, irritability, hair loss, diarrhea, muscle wasting, and poor wound healing (Aills et al, 2008).
Consuming vitamins and minerals in their most natural form (i.e. food) is most ideal, due to the increased bioavailability. However, as post-op WLS patients know, it is sometimes difficult to get in enough protein in a day, let alone eat enough fruits, vegetables, whole grains, dairy, and nuts in order to meet all of the recommended levels of vitamins and minerals. This is why post-op patients are highly recommended to take vitamin/mineral supplements.
Total Vitamin/Mineral Recommended Daily Intake

In order to meet the above values for post-op WLS patients, the ASMBS recommends the following amounts in your bariatric supplements:
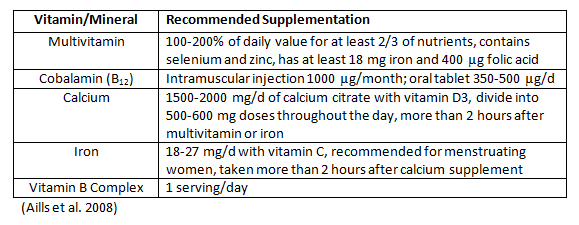
At the end of the day, it doesn’t matter (as much) what kind of supplement you take. What matters most is that you take it consistently and that you verify with your doctor that the supplements are working as they should. Obviously, it makes more sense to take a product designed for the unique needs of a post-operative bariatric patient, but if you don’t take the supplement consistently, it doesn’t matter how optimal it is.
References
- Aills L, Blankenship J, Buffington C, et al. ASMBS Allied Health Nutritional Guidelines for the Surgical Weight Loss Patient. Surgery for Obesity and Related Diseases. 2008;4:S73-S108.
- Frank L. Bariatric Beriberi: Thiamin Deficiency in the Bariatric Patient. Bariatric Times. 2011;8(1):14
 | ABOUT THE AUTHOR Bec McDorman, MS, RDN discovered her passion for health and wellness after undergoing Roux-en-Y Gastric Bypass surgery in 2010 to lose more than 100lbs. Bec has received her masters from Cal Poly Pomona and completed her dietetic internship at Johns Hopkins Bayview Medical Center. She has reached her goal of being a registered dietitian so she can help pre- and post-op bariatric patients with their journey.Read more articles by Bec! |
About the author
Bec McDorman, BS, RYT
Bec McDorman, MS, RDN discovered her passion for health and wellness after undergoing Roux-en-Y Gastric Bypass surgery in 2010 to lose more than 100lbs. Bec has received her masters from Cal Poly Pomona and completed her dietetic internship at Johns Hopkins Bayview Medical Center. She has reached her goal of being a registered dietitian so she can help pre- and post-op bariatric patients with their journey.


