
PuggyDawn S.
All a Newbie would want to know
Jan 30, 2010
I copied this from MSN and thought with the same questions asked on the board over and over...these articles could help!!!
Newbies...bookmark this and save it to your computer so you can always go back and reference it. Then maybe you can pass on the information to someone else wondering about RNY...Pay it forward ~ baby!!
Gastric bypass surgery: What can you expect?
Gastric bypass surgery overview details the surgical procedure, risks, complications and possible weight-loss results.
From MayoClinic.com
Find more |
Weight-loss (bariatric) surgery changes the anatomy of your digestive system to limit the amount of food you can eat and digest. The surgery aids in weight loss and lowers your risk of medical problems associated with obesity.
Gastric bypass is the favored bariatric surgery in the United States. Surgeons prefer this surgery because it's safer and has fewer complications than other available weight-loss surgeries. It can provide long-term, consistent weight loss if accompanied with ongoing behavior changes.
Gastric bypass isn't for everyone with obesity, however. It's a major procedure that poses significant risks and side effects and requires permanent changes in your lifestyle. Before deciding to go forward with the surgery, it's important to understand what's involved and what lifestyle changes you must make. In large part, the success of the surgery is up to you.
How is gastric bypass surgery done?
In gastric bypass (Roux-en-Y gastric bypass) the surgeon creates a small pouch at the top of your stomach and adds a bypass around a segment of your stomach and small intestine.
The surgeon staples your stomach across the top, sealing it off from the rest of your stomach. The resulting pouch is about the size of a walnut and can hold only about an ounce of food. The pouch is physically separated from the rest of the stomach. Then, the surgeon cuts the small intestine and sews part of it directly onto the pouch.
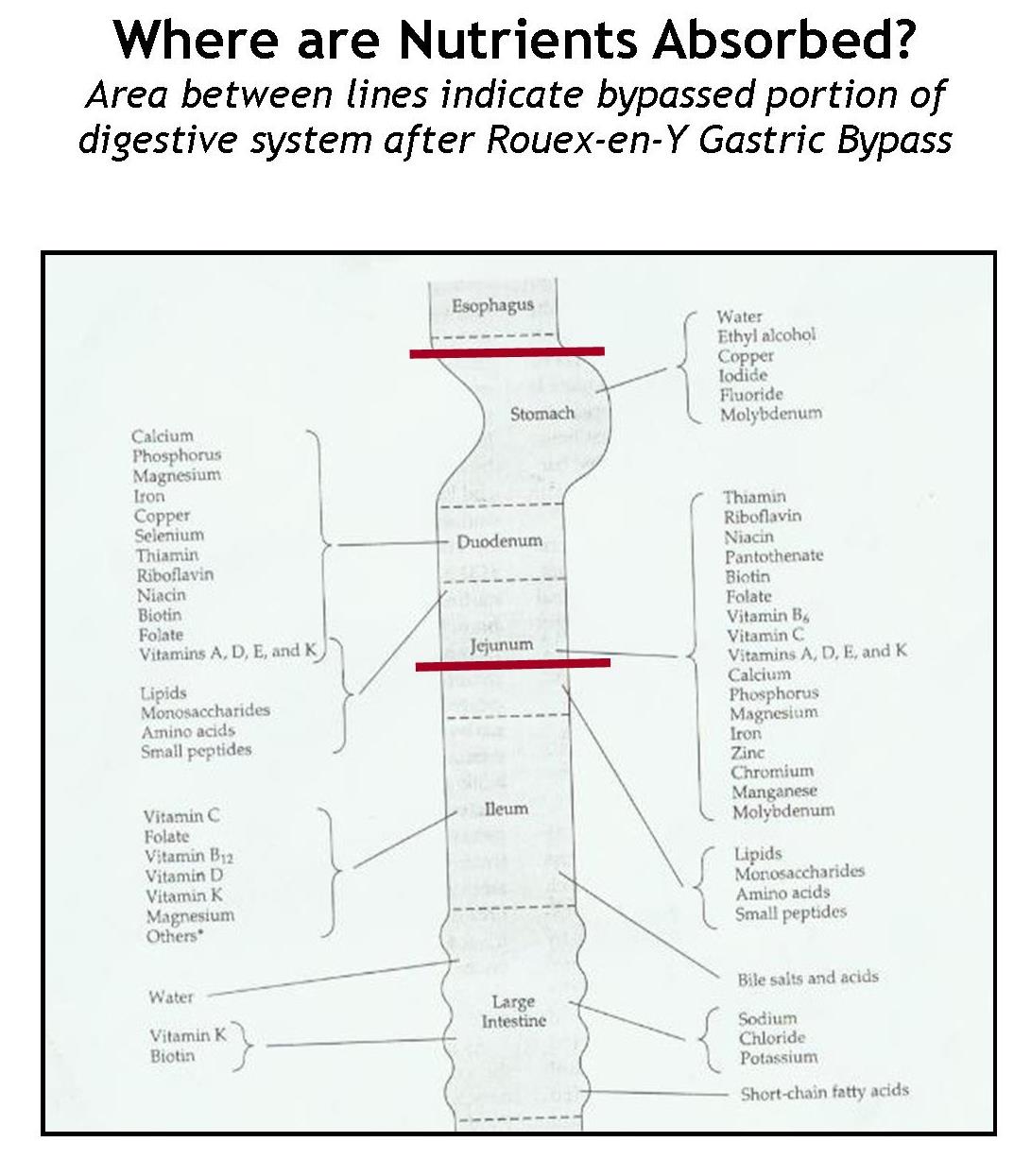
This connection redirects the food, bypassing most of your stomach and the first section of your small intestine, the duodenum (doo-o-DEE-num). Food enters directly into the second section of your small intestine, the jejunum (jay-JOO-num), limiting your ability to absorb calories. Even though food never enters the lower part of your stomach, the stomach stays healthy and continues to secrete digestive juices to mix with food in your small intestine.
Some surgeons perform this operation by using a laparoscope — a small, tubular instrument with a camera attached — through short incisions in the abdomen (laparoscopic gastric bypass). The tiny camera on the tip of the scope allows the surgeon to see inside your abdomen.
Compared with traditional "open" gastric bypass, the laparoscopic technique usually shortens your hospital stay and leads to a quicker recovery. Fewer wound-related problems also occur. Not everyone is a candidate for laparoscopic gastric bypass, however. Talk to your doctor about whether this approach is appropriate for you.
Image
Image of gastric bypass surgery

Before gastric bypass, food (see arrows) enters your stomach and passes into the small intestine. After surgery, food is redirected so that it bypasses (see shaded areas) most of your stomach and the ...
Enlarge Image
What can you expect during the surgery?
Gastric bypass surgery is performed under general anesthesia. This means you inhale analgesics as a gas or receive the anesthetic agent through an intravenous (IV) line so that you're asleep during the surgery.
During surgery, a tube is passed through your nose into the upper stomach pouch. Occasionally, this tube stays in overnight. The tube is connected to a suction machine after surgery to keep the small stomach pouch empty so that the staple line can heal.
You may have another tube in the bypassed stomach. This tube comes out the side of your abdomen and is removed four to six weeks after surgery. Some skin irritation may develop around this tube.
Gastric bypass surgery takes about four hours. After surgery, you wake up in a recovery room, where medical staff will monitor you for any complications. Your hospital stay may last from three to five days.
What can you expect after gastric bypass surgery?
You won't be allowed to eat for one to three days after the surgery so that your stomach can heal. Then, you'll follow a specific progression of your diet for about 12 weeks. The progression begins with liquids only, proceeds to pureed and soft foods, and finally to regular foods.
With your stomach pouch reduced to the size of a walnut, you'll need to eat very small meals during the day. In the first six months after surgery, eating too much or too fast may cause vomiting or an intense pain under your breastbone. The amount you can eat gradually increases, but you won't be able to return to your old eating habits.
You may experience one or more of the following changes as your body reacts to the rapid weight loss in the first three to six months:
- Body aches
- Feeling tired, as if you have the flu
- Feeling cold
- Dry skin
- Hair thinning and hair loss
- Mood changes
What are the benefits of gastric bypass surgery?
Within the first two years of surgery, you can expect to lose 50 percent to 60 percent of your excess weight. If you closely follow dietary and exercise recommendations, you can keep most of that weight off long term.
In addition to dramatic weight loss, gastric bypass surgery may improve or resolve the following conditions associated with obesity:
- Type 2 (adult-onset) diabetes
- High blood pressure
- High blood cholesterol
- Obstructive sleep apnea
- Gastroesophageal reflux disease (GERD)
The improvements observed in type 2 diabetes, high blood pressure and high blood triglycerides may significantly decrease the risk of cardiovascular events in people who have undergone gastric bypass surgery compared with those people who did not have surgery. Also, gastric bypass surgery may reduce the risk of dying of diabetes, heart disease and cancer. The surgery has also shown to improve mobility and quality of life for people who are severely overweight.
What are the risks of gastric bypass surgery?
As with any major surgery, gastric bypass carries risks such as bleeding, infection and an adverse reaction to the anesthesia. Possible risks specific to this surgery include:
- Death. A risk of death has been associated with gastric bypass surgery. It has generally been reported to be one death per 200 to 300 surgeries. Higher risks have been reported amongst Medicare recipients. The risk varies depending on age, general health and other medical conditions. Talk to your doctor about the exact level of risk gastric bypass surgery may pose for you.
- Blood clots in the legs. Blood clots in the legs are more likely to occur in very overweight people. Blood clots can be dangerous. In some cases, they travel to the lungs and lodge in the lungs' arteries causing a pulmonary embolism — a serious condition that damages lung tissue and can lead to death. Walking and using leg wraps that apply intermittent pressure to the leg can help reduce this risk of blood clots in the legs. Smoking has been shown to increase the risk of clotting in people undergoing gastric bypass surgery. Quitting smoking is strongly recommended.
- Leaking at one of the staple lines in the stomach. This severe postoperative problem is treated with antibiotics. Many cases heal with time. Often, however, the leak can be serious enough to require emergency surgery.
- Incision hernia. An incision hernia is a weakness in the incision. This is more likely to occur if you have an open procedure and a large abdominal incision. This usually requires surgical repair, depending on the symptoms and the extent of the hernia.
- Narrowing of the opening between the stomach and small intestine. This rare complication may require either an outpatient procedure — in which a tube is passed through your mouth to widen (dilate) the narrowed opening — or a corrective surgery.
- Dumping syndrome. This is a condition where stomach contents move too quickly through the small intestine, causing nausea, vomiting, diarrhea, dizziness and sweating. It's frequently experienced after eating sweets or high-fat foods.
Other potential complications of gastric bypass surgery include:
- Vitamin and mineral deficiency (iron deficiency anemia, vitamin B-12 deficiency and vitamin D deficiency)
- Dehydration
- Gallstones
- Bleeding stomach ulcer
- Intolerance to certain foods
- Kidney stones
- Low blood sugar (hypoglycemia) related to excessive insulin production
What are other weight-loss surgery options?
Though it's the most commonly used, gastric bypass is just one kind of weight-loss surgery. Other types include:
- LAP-BAND adjustable gastric banding (LAGB). The surgeon uses an inflatable band to partition the stomach into two parts by wrapping the band around the upper part of your stomach. Pulling it tight like a belt, the surgeon creates a tiny channel between the two pouches. The band keeps the opening from expanding and is designed to stay in place indefinitely. It can be adjusted or surgically removed if necessary. LAGB is gaining popularity because it's a simpler procedure and has a lower complication rate when compared with more-involved procedures. However, LAGB causes less weight loss and a slower rate of weight loss than does the Roux-en-Y gastric bypass. This surgery isn't recommended for people who have certain medical conditions, such as Crohn's disease, large hiatal hernias or a history of gastric ulcers.
- Vertical banded gastroplasty. This operation, also referred to as stomach stapling, divides the stomach into two parts — limiting space for food and forcing you to eat less. There is no bypass. Using a surgical stapler, the surgeon divides your stomach into upper and lower sections. The upper pouch is small and empties into the lower pouch — the rest of your stomach. Partly because it doesn't lead to adequate long-term weight loss, this weight-loss surgery has fallen out of favor.
- Biliopancreatic diversion with duodenal switch. In this procedure, the surgeon removes about 80 percent of the stomach. The valve that releases food to the small intestine is left along with a limited portion of the small intestine that normally connects to the stomach (duodenum). The surgery bypasses the majority of the intestine by connecting the end portion of the intestine to the duodenum near the stomach. This weight-loss surgery offers sustained weight loss, but it presents a greater risk of malnutrition and vitamin deficiencies and requires close monitoring. It's generally used for people who have a body mass index greater than 50.
content by:

Gastric bypass diet: What to eat after weight-loss surgery
Gastric bypass diet — recommendations on what you can eat after weight-loss surgery.
From MayoClinic.com
Find more |
What you eat, how you eat and how much you eat changes after gastric bypass surgery — surgery that alters the anatomy of your digestive system to promote weight loss.
With your stomach pouch reduced to the size of a walnut or small egg and portions of your small intestine bypassed, you'll need to follow a specific diet after gastric bypass surgery. A registered dietitian can assist you in creating this gastric bypass diet, which includes what type and how much food to eat with each meal and the required consistency and texture of the food. Closely following your gastric bypass diet promotes healthier weight loss and better nutrition.
After surgery: The first three months
You won't be allowed to eat for one to two days after the surgery. Then you consume specific foods according to a diet progression. The purpose of the gastric bypass diet progression is to help in the healing process, minimize stress on surgical sites and allow time for your body to adapt to the new eating patterns.
The following are common phases in the gastric bypass diet progression:
- Liquids — foods and fluids that are liquid or semiliquid at room temperature and contain mostly water, such as broth, juice, milk, strained cream soup and cooked cereal. In most cases, you stay on a liquid diet for one to two days.
- Pureed foods — foods with a consistency of a smooth paste or a thick liquid. Pureed foods contain no distinct pieces. The pureed diet is generally followed for three to four weeks, or as recommended by your dietitian or doctor.
- Soft foods — foods that are tender and easy to chew, such as ground or finely diced meats, canned or soft, fresh fruit, and cooked vegetables. You usually eat soft foods for eight weeks before progressing to eating foods of regular consistency with firmer texture as recommended by your dietitian or doctor.
During the diet progression, you eat many small meals a day and sip liquids slowly throughout the day (not with meals). You might first start with six small meals a day, then progress to four meals and finally, when following a regular diet, decrease to three meals a day. Typically, each meal includes protein-rich foods, such as lean meat, low-fat dairy products (yogurt, cheese) or eggs. Protein is important for maintaining and repairing your body after surgery.
How quickly you move from one step to the next depends on how fast your body adjusts to the change in eating patterns and the texture and consistency of food. People usually start eating regular foods with a firmer texture three months after surgery, but it can occur sooner.
Lifelong changes: New eating habits
The changes in your digestive system restrict how much you can eat and drink with each meal. To avoid problems and to ensure you're getting nutrients you need, closely follow these guidelines:
- Eat small amounts. Just after surgery, your stomach holds only about 1 ounce of food. Though your stomach stretches over time to hold more food, by the end of three months, you may be able to eat 1 to 1 1/2 cups of food with each meal. Eating too much food not only adds more calories than you need but also may cause pain, nausea and vomiting. Make sure you eat only the recommended amounts and stop eating before you feel full.
- Eat and drink slowly. Eating or drinking too quickly may cause dumping syndrome — when foods and liquids enter your small intestine rapidly and in larger amounts than normal, causing nausea, vomiting, diarrhea, dizziness and sweating. To prevent dumping syndrome, choose foods and liquids low in fat and sugar, eat and drink slowly, and wait 30 minutes before or after each meal to drink liquids. Take at least 30 minutes to eat your meals and 30 to 60 minutes to drink 1 cup of liquid. Avoid foods high in fat and sugar, such as regular soda, candy and candy bars, and ice cream.
- Chew food thoroughly. The new opening that leads from your stomach into your intestine is very small, and larger pieces of food can block the opening. Blockages prevent food from leaving your stomach and could cause vomiting, nausea and abdominal pain. Take small bites of food and chew them to a pureed consistency before swallowing. If you can't chew the food thoroughly, don't swallow it.
- Drink liquids between meals. Drinking liquids with your meals can cause pain, nausea and vomiting as well as dumping syndrome. Also, drinking too much liquid at or around mealtime can leave you feeling overly full and prevent you from eating enough nutrient-rich foods. Expect to drink at least 6 to 8 cups (48 to 64 ounces) of fluids a day to prevent dehydration.
- Try new foods one at a time. After surgery, certain foods may cause nausea, pain, vomiting or may block the opening of the stomach. The ability to tolerate foods varies from person to person. Try one new food at a time and chew thoroughly before swallowing. If a food causes discomfort, don't eat it. As time passes, you may be able to eat this food. Foods and liquids that commonly cause discomfort include meat, bread, pasta, rice, raw vegetables, milk and carbonated beverages. Food textures not tolerated well include dry, sticky or stringy foods.
- Take recommended vitamin and mineral supplements. After surgery, your body has difficulty absorbing certain nutrients because most of your stomach and part of your small intestine are bypassed. To prevent a vitamin or mineral deficiency, take vitamin and mineral supplements regularly. These generally include a multivitamin-multimineral, calcium, iron, vitamin B-12 and vitamin D. Talk to your health care provider about recommended vitamin and mineral supplements following gastric bypass surgery.
Weight loss and weight gain
Within the first two years following surgery, you can expect to lose 50 percent to 60 percent of your excess weight, if you follow the dietary and exercise recommendations. If you continue to follow these recommendations, you can keep most of that weight off long term.
People who regain weight after gastric bypass surgery usually are consuming too many high-calorie foods and beverages and don't exercise enough. And rather than eating three meals a day and perhaps a planned healthy snack, some people engage in a grazing-type eating pattern — eating food all day long. Grazing often leads to consuming too many calories, which causes weight gain.
Successful weight management requires the following healthy habits:
- Limit or avoid high-sugar, high-fat foods, which provide many calories but few nutrients.
- Minimize unplanned snacking or frequent grazing, which increases calorie intake.
- Exercise regularly.
- Take the recommended vitamin and mineral supplements.
- Attend regular follow-up appointments with your health care provider to review your symptoms and progress and to make sure you don't have any vitamin or mineral deficiencies.
If you aren't losing weight or are regaining weight after surgery, see your doctor. He or she can help assess your eating behaviors and exercise habits and help you confront and overcome any weight-loss obstacles.
Though weight-loss surgery helps you shed the pounds, its success depends on your willingness to adopt lifelong healthy-eating and exercise habits. What you eat and how you eat changes after surgery, but the benefits of weight loss and your improved health are well worth these efforts.
content by:Gastric bypass surgery: Who is it for?
Gastric bypass surgery — Find out if you're a candidate for this weight-loss surgery.
From MayoClinic.com
Find more |
It's always best to lose weight through a healthy diet and regular physical activity. But if you're among those who have tried and can't lose the excess weight that's causing your health problems, weight-loss (bariatric) surgery may be an option.
Gastric bypass surgery — one type of bariatric surgery — changes the anatomy of your digestive system to limit the amount of food you can eat and digest. Weight loss is achieved by restricting the amount of food that your stomach can hold and by reducing the amount of calories that are absorbed.
Gastric bypass surgery isn't for everyone, however. It's a major procedure that poses significant risks and side effects and requires permanent changes in your lifestyle. An extensive and careful screening process determines whether you're a candidate for this surgery.
Gastric bypass surgery criteria
Generally, gastric bypass surgery is reserved for people who are unable to achieve or maintain a healthy weight through diet and exercise, are severely overweight, and who have health problems as a result. Gastric bypass surgery may be considered if:
- Your body mass index (BMI) is 40 or higher (extreme obesity)
- Your BMI is 35 to 39.9 (obesity), and you have a serious weight-related health problem, such as diabetes or high blood pressure
Gastric bypass surgery doesn't replace the need for following a healthy diet and regular physical activity program. In fact, the success of the surgery depends in part on your commitment to following the guidelines given to you about diet and exercise. As you consider weight-loss surgery, make sure that you make every effort to exercise more, change your eating habits and adjust any other lifestyle factors that have contributed to your excess weight.
Before surgery: The screening process
Surgical candidates must go through an extensive screening process. Not everyone who meets the criteria for gastric bypass surgery is psychologically or medically ready for the surgical procedure. A team of professionals, including a physician, dietitian, psychologist and surgeon, evaluates whether weight-loss surgery is appropriate for you. This involves identifying which aspects of your health might improve after surgery and which aspects of your health may increase the risks of surgery. Surgery is recommended when the perceived benefits of surgery outweigh the recognized risks.
Your willingness and ability to follow through with the recommendations made by your health care team and to carry out prescribed changes in your diet and exercise routine help determine your readiness for surgery. The surgery may not be recommended or may be postponed if there's concern that you aren't psychologically or medically ready for such surgery.
It's important to follow your doctor's directions in preparing for gastric bypass surgery. These may include restrictions on eating and drinking, limiting or stopping the use of nicotine products, and starting a physical activity program.
Surgery may be delayed or canceled if:
- There is concern that you're not psychologically or medically ready for surgery
- You haven't made appropriate changes in your lifestyle
- You've gained weight during the evaluation process
Financial concerns
Once you've completed the screening process and your surgeon determines you're a candidate for gastric bypass surgery, you need to secure financial preapproval from your medical insurance company, Medicare or state assistance. The preapproval process requires documentation from your team of doctors that demonstrates a medical need for the procedure. It usually takes several weeks to receive approval.
Requirements for proving medical necessity for weight-loss surgery vary among insurers. Check to see what related services are covered, for example, pre-evaluation appointments and follow-up appointments after surgery. You may have to pay some of the costs yourself.
The process of securing financial resources and then being scheduled for surgery can take several months. The long approval process allows you time to make a final decision about the surgery. Surgery usually isn't scheduled until insurance or other financial coverage is established.
Looking ahead
Surgery for weight reduction isn't a miracle procedure. It doesn't guarantee that you'll lose all of your excess weight or that you'll keep it off long term. Weight-loss success after gastric bypass surgery depends on your commitment to making lifelong changes in your eating and exercise habits. But the feeling of accomplishment as you lose weight and your improved health are significant benefits and are well worth your efforts.
content by:I just thought this infromation was too good to let slide by....
Dawn
Which calcium??
Sep 22, 2009
Calcium Citrate vs. Calcium Carbonate
After RNY our pouch no longer produces gastric acid (scientifically known as hydrocloric acid). And after surgery most surgeons have their patients take a proton pump inhibitor for several weeks/months after surgery to "kill of" any remaining acid producing cells that might cause ulcers. I took Prevacid for 12 months post-op.
The diagnosis for lack of gastric acid in a patients stomach is called Achlorhydria. This disorder is often seen in elderly patients, but since WLS has become increasingly popular, doctors have recognized that RNY patients need the same alternative treatment as elderly patients who have the same diagnosis.
Calcium carbonate requires gastric acid in order to break down and be used by the body. It does not break down in a neutral pH environment -- meaning it is not water soluable, it requires a highly acid environment to be bioavailable.
Calcium citrate is water soluable and dissolves quickly and easily in a neutral pH environment. No acid is required. In fact, a calcium citrate supplement tablet will dissolve in plain water in about 5 to 10 minutes.
It means that after RNY we must use calcium citrate as our calcium supplementation. Calcium carbonate does not dissolve and is not used by our body after WLS. The ASMBS Guidelines for Bariatric Nutrition recommends we take 1500-2000mg of calcium citrate supplement per day in addition to whatever calcium we get from food. It is common knowledge among the medical community that doses of calcium must be no larger than 400-500mg at a time, spaced at least 2 hours apart.
Tums, Viactiv, Caltrate and the generic versions of all these brands..... all are calcium carbonate. Stay away from them. Look for Citracal, Bariatric Advantage, UpCalD, TwinLabs Calcium Citrate and others. Read the label carefully not only for the type of calcium, but also for the serving size. Many calcium citrate brands require 2 pills per dose, so do the math according to your daily requirements. For instance, Citracal Petites have 200mg calcium per pill... so to get 2000mg of calcium per day you'll need 10 pills in 5 doses throughout the day.
(thanks Pam)
When to take which vitamin?
Sep 13, 2009
All supplements are D3....many companies leave the '3' off the label. If behind the 'D" it say cholecalciferol, it is D3. If it says ergocaldiferol it is D2 which is not as aborbable as D3 therefore companies generally don't use it.
Most Vitamin D supplements on the market are D3 because D2 isn't as absorbable... but D2 is the only vegetarian Vitamin D (which is the only choice for Vegans and some other dietary requirements) while D3 is from an animal source, typically
whether it is Cholecalciferol (typically from Lanolin, which is sheep's wool) or from Fish Liver Oil, those are the main sources for Vitamin D3.
Iron and Vitamin C are Friends --- Iron needs an acid environment to break down and Vitamin C does that job so make sure they are in your tummy at the same time. Iron does not like food, so take it on an empty stomach. However, if you get an upset tummy because of the iron, pick a non-dairy snack.
Iron and Calcium are Enemies --- iron and calcium fight for the same cell receptors in the body and calcium is bigger and badder and always wins. Which means the iron is simply excreted from the body and not used at all. Keep iron and calcium at least 2 hours apart from each other.
Vitamin B's are a Family --- they work together as a team and are best taken at the same time. Your Multi-Vitamin has many B's in it, so take it together with your biotin, B12 and B-complex if you're taking those too.
(a thank you to Pam)
which labs to get......
May 24, 2009
common question is "which labs?" And "how can I get my insurance company to pay for the lab draws?"
- COMPREHENSIVE METABOLIC PROFILE (sodium, potassium, chloride, glucose, BUN, creatinine, calcium, total protein, albumin, total bilirubin,alkaline phosphatase, aspartate aminotransferase) (Nc,K,C1,CO2,Glu,BUN,Cr,Ca,TP,Alb,Tbili,AP,AST,ALT)
- LIPID PROFILE (cholesterol, HDL, LDL, triglycerides, chol/HDL ratio) (Fasting specimen) , Tchol,Trig,HDL,Calc,,LDL)
- ALT (SPGT)
- GGT (important if liver, renal or pancreatic issues are suspected)
- LDH PHOSPHORUS – INORGANIC
- URIC ACID (usually used to determine if a patient has gout)
- CBC (HEMOGRAM/PLT/DIFF)
- B-12 & FOLATE - and HOMOCYSTEINE
- IRON, TIBC, % SAT AND FERRITIN (very important)
- VITAMIN A & D (25-hydroxy)
- THYROID PANEL (T3U, T4, FTI, TSH)
- SERUM INTACT PTH PARATHYROID
- THIAMINE (B1)
- COPPER
- ZINC
- MAGNESIUM
- RBC
- A1C
- YEARLY - DEXA SCAN for bone density (same time of year).
Possible diagnosis codes:
- 244.9 hypothyroidism
- 250.0 diabetes
- 265.0 Beriberi
- 265.1 Other and Unspecificed Manifestations of Thiamine Deficiency (B1)
- 266.2 cyanocobalamin deficiency (B12)
- 268 vitamin D deficiency
- 268.2 metabolic bone disease
- 269.2 hypovitaminosis
- 269.3 zinc deficiency
- 272.0 hypercholesterolemia
- 275.40 calcium deficiency
- 276.9 electrolyte and fluid disorders
- 280.9 iron-deficiency anemia
- 281.0 pernicious anemia
- 281.1 other B12 deficiency anemia
- 281.2 folate deficiency anemia
- 285.9 anemia, unspecified
- 401.9 hypertension
- 579.3 post-surgical malabsorption
- 579.8 intestinal malabsorption
Protein: 7's
Albumin: 4's
Pre-Albumin: 20-30's
Iron: 80-100
Ferritin: 200-300
HGB: 12+
HCT: 36+
Vit A: 60- 80
Vit D: 80-12 0
Calcium: 9.0-9.4
PTH: 20-40
Vit B1: Mid to top of range
Vit B6: Mid to top of range
Magnesium: Mid range (but also go by if we have leg/foot cramping)
Zinc: Mid range
Vit B12: 1000 +
Folate: Top of range
AST (sgot): Below 40 A
LT (sgpt): Below 40
absorption of psych meds after RNY
Apr 07, 2009
I am bipolar and I thought this chart would help others with bipolar disorder that are worried about the absorption rate of their psych meds after surgery.
I've had to have several medication changes after RNY surgery because of issues of absorption. If you have questions, please print the chart out and take it with you at your next doctor's appt.

Twelve of the 22 medication preparations were found to dissolve differently across the two environments. Ten of the 12 dissolved more in the control model, and only two dissolved to a greater degree in the RYGB model. Although not reported, variability within each sample of three pills was minimal. In no case did a value stray beyond 10% difference from the median weight change. (Variability data are available from the authors.) We chose not to report standard deviations, as we could not confirm that the data were parametric. Reporting the high and low values in addition to the median seemed unhelpful, considering that there were only three pills in each sample.
Within the antidepressant class, bupropion was the only agent that dissolved to a greater degree in the RYGB model (a median of 450 mg dissolved, compared with 320 mg in the control model, p<0.05). The dissolution of citalopram and venlafaxine did not differ between conditions. The remaining antidepressant medications (amitriptyline, fluoxetine, paroxetine, sertraline) dissolved more in the control model than in the RYGB model (Table 1).
Among the anxiolytic/sedatives, only one of the six medications varied between the conditions. Clonazepam was found to dissolve slightly more in the control model (a median of 100 mg dissolved, compared with 90 mg in the RYGB model, p<0.05). Dissolution of the remaining agents (buspirone, diazepam, lorazepam, trazodone, zolpidem) did not differ between conditions (Table 1).
For the antipsychotic/miscellaneous category, lithium carbonate dissolved significantly more in the RYGB model (median of 280 mg dissolved, compared with 130 mg in the control model, p<0.05). The dissolution of haloperidol, oxcarbazepine, and methylphenidate did not vary between conditions. Five newer antipsychotics (clozapine, olanzapine, quetiapine, risperidone, and ziprasidone) had greater dissolution in the control condition (Table 1).
Famous people who have had gastric-bypass
Apr 07, 2009
Gastric Bypass:
- Patti Austin
- roux-en-y, 2004
- American R&B and jazz singer, known for hits like Do You Love Me? / The Genie and Baby, Come To Me.
- Rosanne Barr
- Fobi pouch, 1998
- sometimes controversial American comedian and actress who gained fame with her stand-up act and acheived super-stardom with her hit show Roseanne.
- Kent "Big Boy" Alexander
- duodenal switch, 2003
- Los Angeles morning radio DJ. Morning DJs on American radio (especially in big cities) can become nationally famous, as is the case with Big Boy. He once appeared almost nude on a billboard in L.A. - when he was almost 500 pounds.
- Darlene Cates
- vertical banded gastroplasty, 1984 (the old-fashioned "stomach stapling")
- American actress best known for playing "Momma" in the film What's Eating Gilbert Grape. She weighed a little over 400 pounds at the time of her surgery and lost about 100 pounds in the year following surgery. She subsequently gained back the 100 pounds plus at least 100 more. She says she regrets having the surgery and does not wish to have a revision. We find her story particularly poignant. She has struggled with her weight nearly all of her life - like so many of us. We think it's important that we learn from both the good stories and the bad when it comes to obesity surgery.
- Andrae and Sandra Crouch
- Fobi pouch, 2003 or earlier
- American gospel singers and twins. Andrae is quite famous in the U.S. gospel genre.
- Michael Genadry
- roux-en-y, 2002
- American actor, one of the stars of the television dramedy Ed. His surgery was actually written into the storyline to explain his rapid weight loss.
- Gil Gerard
- mini-gastric bypass, 2006
- American actor famous for playing Buck Rogers on television from 1979-1981. He allowed the Discovery Channel to follow his obesity surgery journey, a show which aired in 2007.
- Adam Goldstein
- roux-en-y, 2003
- Club DJ and former boyfriend of Nicole Ritchie.
- Jackie Guerra LOOK in my pics ~ to the left, I've met her...she was a speaker at an OH conference!!
- gastric bypass (RNY), 2003
- Emmy Award-winning American comedienne, Actress, Author, and Jewelry Designer. She played Selena's sister in the film Selena, had a sitcom called First Time Out, and a show on the DIY network called Jewelry Making.
- Jennifer Holliday
- Fobi pouch, 1989-1990
- American actress and singer. She won a Tony award in 1982 for Best Lead Actress in a Musical for Dreamgirls. She won a Grammy that same year for the song And I Am Telling You I'm Not Going, also from Dreamgirls. Interestingly, She says in a 1991 Ebony article that she lost 148 pounds by going on a liquid diet. Dr. Fobi lists her as a Fobi pouch patient though, so we wonder when exactly she had surgery, and if she just didn't want to reveal it at first.
- Randy Jackson
- Fobi pouch, 2003
- Most famous as an American Idol judge, he's also a Grammy Award-winning musician.
- Jesse Jackson, Jr.
- gastric bypass (type unknown), revealed in March 2005
- American politician and son of activist and former presidential candidate Jesse Jackson.
- Etta James
- Fobi pouch, 2003
- American blues/jazz singer and songwriter, most famous for the 1961 song At Last. (one of our favourite songs!)
- Star Jones
- roux-en-y, 2003
- These days we think she is most famous for denying that she had gastric bypass, even though she so obviously lost weight at a dramatic pace when she was one of the hosts of the American television show The View. She finally admitted to having undergone obesity surgery in the August, 2007 issue of Glamour magazine.
- Harry Lee
- roux-en-y, 2003
- He's not necessarily famous in the Hollywood way, but he is a person of note. He was a Chinese-American politician who was elected Sheriff of Jefferson Parish (where New Orleans is) in Louisiana six times, serving over 27 years and had a career full of controversy. He was known for "telling it like it is", although not everyone always appreciated his style. The day before hurricane Katrina hit New Orleans he went on the radio and said, "You better haul ass! Y'all should have left yesterday." A true statement, albeit said with some indelicacy. He died from Leukemia in October 2007, just three weeks before his expected re-election to office.
- Ron Lester
- gastric bypass (type unknown), 2001
- American comedian and actor. He played Billy Bob in the film Varsity Blue, and parodied that role in Not Another Teen Movie. He lost 348 pounds with gastric bypass surgery, an incredible amount of weight. He has reportedly had ten plastic surgery procedures to remove excess skin.
- Ralphie May
- roux-en-y, 2003
- American comedian who gained fame on the television show Last Comic Standing. He won first runner up in the competition, and has since made a comedy CD, did a special on Comedy Central, and makes regular guest appearances on popular comedy radio shows. He was a true heavyweight, tipping the scales at over 800 pounds at his heaviest. In mid-2007 his weight was reportedly in the 300's.
- JoMarie Payton
- Fobi pouch, 2003 or earlier
- American actress most famous for her role as Harriette Winslow (the mom) on the sitcom Family Matters.
- John Popper
- roux-en-y, 2000
- American singer and songwriter. He's the frontman for the group Blues Traveler, and is amazing on the harmonica. Who knew the humble harmonica could be such a beautiful instrument? He had a near heart attack in 1999 at the tender age of 32. He had an emergency angioplasty which revealed that he had 95% arterial blockage.
- Anne Rice
- roux-en-y, 2003
- This American author has a huge following for her book series The Vampire Chronicles, which includes the stunningly successful Interview with a Vampire (later made into a movie starring Tom Cruise, Brad Bitt and Kirsten Dunst). Although she was a self-proclaimed athiest most of her adult life, she returned to her Roman Catholic roots around the time of the death of her husband of 41 years, Stan. She announced in 2005 that she would henceforth write "only for the Lord" and declared most strongly that she would not be writing any more vampire novels, much to the dismay of her fans. In 1998 she discovered that she had Type 1 diabetes after she fell into a diabetic coma. After her husband's death in 2002, her weight rose steadily, and she suffered from sleep apnea "and other weight-related problems", which led her to undergo gastric bypass surgery.
- Al Roker
- roux-en-y, 2002
- Anchor on the American morning news show "Today". Al Roker was one of the first people we remember talking about gastric bypass surgery. We were amazed at the way he seemed to shrink in front of our eyes every day. He seems lately to have gained back a fairly substantial amount of weight. Another example that this surgery is not a cure-all!
- Lulu Roman
- gastric bypass (type unknown), year unknown
- Gospel singer and American actress from the long running comedy-music series Hee-Haw.
- Glenn Shadix
- roux-en-y, 2000
- American actor known for his deep voice and southern accent. He is known for playing Otho in the film Beetlejuice, and does a lot of voice work for animated television shows and movies.
- Deborah Voigt
- roux-en-y, 2005
- An American opera singer. Deborah has expressed some concerns about how her weight loss might have affected her voice. In an 2006 interview with Opera News she asserts that her diaphragm function and voice are not compromised, but she does say, "I do have to think about it more now. I have to remind myself to keep my ribs open. I have to remind myself, if my breath starts to stack. When I took a breath before, the weight would kick in and give it that extra Whhoomf! Now it doesn't do that."
- Charlie Weis
- roux-en-y, 2002
- Head coach of the American football team for the University of Notre Dame. He sued his doctors for damages due to complications from his obesity surgery, during which he almost died. He checked into the hospital under an assumed name hoping to keep the surgery quiet, but the malpractice lawsuit has put every detail of his weight struggle in the public eye. In his book, No Excuses: One Man's Incredible Rise Through the NFL to Head Coach of Notre Dame, he says that having gastric bypass "was probably the biggest mistake of my life." He initially lost 100 pounds, but says he has gained back about 50.
- Basil White
- roux-en-y, 2000
- An American comedian (lots of comedians on this list - we wonder whether that's a coincidence. How many of us have tried to use humour to cover our pain at being obese?). He kept a detailed diary of his experience.
- Carnie Wilson
- roux-en-y, 2000
- She's been so public about her struggle with obesity, her gastric bypass surgery, and her subsequent struggles that we hardly know where to begin! She is the daughter of Beach Boys singer Brian Wilson and his first wife Marilyn Rovell. She was part of the popular pop singing trio Wilson Phillips. She speaks of how humiliating it was to be "the fat one" in this sucessful group. Her surgery was broadcast live on the Internet, she lost 150 pounds, went on to pose for Playboy and wrote the book that changed The Guru's life: Gut Feelings.