Malabsorbtion RNY VS. DS
I have begun my 6 month diet/exercise program for insurance purposes and have chose RNY as my surgery type as of now, but, I have been researching DS. Now forgive me if I sound ignorant, I just started researching the DS surgery and it is my understanding the only difference, (other than the obvious difference in the surgeries themselves), is that with the DS there is less risk of develping hypoglycemia, or I think it's called Reactive Hypoglycemia>>>????
Because of the way the surgery is performed on the pyloric valve. Both surgeries have malabsorbtion and restriction. Can anyone tell me, other than the procedure itself, what the difference is between the two as far as the outcome goes?
Both require supplements for the rest of your life.
Both offer the benefit of restriction.
I do know that there is no "dumping" for people that have the DS and
People that have the DS surgery may have more loose stools, etc.
Is there anything else I should know that is important?
Thanks for all your help~
P.S
I researched the DS awhile back-not a whole lot-because I was told it is a much riskier surgery-but as I have been reading, the stats are almost the same compared to RNY as far as complication, mortality rates, etc. I kind of stopped researching because the surgery is a bit more complicated.

Also the DS offers the best long term resolution for diabetes, see here for details
http://www.obesityhelp.com/forums/diabetes/3751535/If-you-ar e-Type-2-and-considering-WLS/
Lowish BMI? See Lightweights Board! Lightweight Creed For more on DS see www.DSfacts.com
If you don't have peace, it isn't because someone took it from you; you gave it away. You cannot always control what happens to you, but you can control what happens in you John C Maxwell  Sleeve 2010 Dr López Corvala, Mexico. DS 2012 Dr Himpens, Belgium
Sleeve 2010 Dr López Corvala, Mexico. DS 2012 Dr Himpens, Belgium
I ![]() my DS
my DS ![]()

It will help if you look at diagrams of the different anatomy, but I'll try to summarize:
With gastric bypass, a 1 oz pouch is created at the top of your stomach, and the small intestine is attached to the pouch. Nothing is removed, which means the rest of the stomach remains as the "blind stomach", meaning it can't be seen with endoscopy or upper GI x-rays. The pyloric valve is still there, it just isn't in use. The entire duodenum and just a little bit of the next part of the small intestine are bypassed.
With the DS, a sleeve gastrectomy is done, with roughly 75-80% of the stomach removed, leaving a sleeve shaped stomach of maybe 3-4 oz (this varies by surgeon). The stomach continues to empty normally through the pyloric valve. The duodenum is divided and about half of the small intestine is bypassed, with the lower half of the small intestine (the ileum) attached to the duodenum and the upper half attached towards the end of the ileum to form the common channel. Again, lengths vary by surgeon.
What does all this mean?
With gastric bypass, you get permanent malabsorption of various vitamins and minerals, but very little caloric malabsorption. With DS, you also get permanent malabsorption of various vitamins (a different assortment) but permanent, significant malabsorption of calories, esp fat calories.
With gastric bypass, you can have dumping and/or reactive hypoglycemia, though not everyone does. These are NOT weight loss tools, they are unpleasant side effects. They rarely occur with DS (I've seen one person say she has dumping). With gastric bypass, you must stick with a low calorie, low carb, low fat diet for life. You cannot take NSAIDs for life. Food can get stuck at the stoma.
With the DS, you need to eat more protein, but can eat fat freely, and you do still have to watch carbs. You can take NSAIDs safely (in proper doses). Food does not get stuck, and you don't have to chew it to a puree.
You are right that the DS is NOT higher surgical risk. This is a myth from the old days when it was reserved for the patients with the highest bmi's and most comorbidities. Of course that group was higher risk and had more complications. The complication rate is the same for either surgery. It is easier to get into trouble with vitamin and/or protein deficiencies with the DS, and anyone considering the DS MUST make the committment to taking their supplements, getting appropriate lab work, and eating plenty of protein for life. It's crucial, but generally not difficult.
Perhaps the biggest different is in the results. The DS has the highest percentage excess weight loss of any wls, and the lowest failure rate. It has the best rate of resolution of almost all comorbidities.
Do keep in mind that not every bariatric surgeon does the DS. There is a list of vetted DS surgeons at dsfacts.com. Any list you find here is not accurate. From where you are, I think the closest would be Dr. Anthone in Omaha, but check the list for yourself.
Larra

In the DS, the pyloric vale remains in its normal position at the exit of the stomach, and still keeps on doing its job, just like it does pre-op. In the RNY, the pylorus is bypassed---it remains a part of the remnant stomach, and does nothing.
In the RNY, the pylorus is replaced by the stoma, a man-made, always-open hole. Normal stomach functions cease---the pouch does NOTHING but store food for a while. Over time, the stoma can stretch, and when that happens, no more restriction. ANd so far, no one's found a really good way of repairing a stretched stoma.
Even when functioning properly, the stoma is the main reason for dumping syndrome---undigested food enters the small intestine in a place where, in normal anatomy, undigested food NEVER goes. In some people, with certain foods, this causes an unnatural insulin reaction that has nasty side effects.
The stoma is also largely responsibe for so-called 'late dumping', more properly known as reactive hypoglycemia. For some people, this never happens. FOr others, it's very mild, and/or easily controlled by diet. FOr others, it's more severe, and while controlled by diet, it requires a VERY strict eating schedule and very strict eating protocol. For some very few people, it's a completely life-altering event.
Loose stools. Well.
This is, for most people, totally diet-based. The more fat one eats, the looser one's stools tend to be, since about 80% of the fat a DSer eats goes down the toilet. How much fat is too much varies from person to person. Too little fat can cause constipation. I'd guess that about 98% of DSers find a happy medium and have comfortable bowel habits.
Loose stools can also be caused by bacterial overgrowth or other medical issues. Sometimes bacterial overgrowth can be cured by probiotics, but sometimes a round of antibiotics are required, followed by probiotics to restore the 'good' bacteria. The other medical issues are so rare and so diverse I'm not going to go into them here.
The most important thing you should know about the difference between the RNY and the DS is the long-term, maintained results. The DS has far better ones. (*grin*) Equally important to ME was that the post-op DS eating plan suited me far better.
Here's a pic of the RNY:
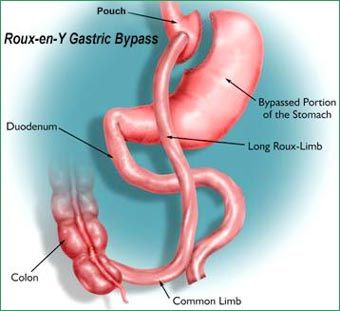

Well, here's a clearer one:

I am just starting my research on the DS and was curious to these statements.
Thank you all again for your help!!
There are far fwr surgeons who are capable of doing a DS than are capable of doing an RNY---and let's face it, the RNY is more profitable.

RNY surgeons keep saying that RNY is the surgery of choice to make folks believe it. They'll make inaccurate statements about the DS and tell you it's not the best surgery for you (hint: they don't do the DS). That's why DSers try to pay it forward letting folks know about the DS and the load of crap that is generally said about the DS. If you want to know about the DS, you need to go to a "REAL" DS surgeon. Read info at DSfacts.com
Most folks have to fight for their DS, chich means that we have researched everything about the DS, talked about it, asked questions here... Generally, we are very well informed about our surgery and our needs after surgery.
Chris
HW/225 - 5'1" ~ SW/205/after surgery 215 ~ CW/145~ BMI-25.8~Normal BMI 132 ~DS Dr Rabkin 4/17/08
Plastics in Monterrey - See Group on OH Dr Sauceda Jan 13, 2011
LBL, BL, small thigh lift, arms & a full facelift on 1/17/11 UBL 1/21/13
Love my Body by Sauceda
Basically the way I understand it you will have less issues with a ds compared to rny, you will be ablr to eat more and bypass more with teh ds compared to rny. It is a more complicated surgery they take out your intestine and measure it and figure out how much to bypass to give you good results. Being able to retain the pyloric valve is really a big deal. A DS can be revised at a later date if need be as well if someone becomes malnurished so to speak they can go back in and readjust it. To me the sleeve part of the surgery is more natural it just makes your stomach smaller instead of giving you a weird little pouch.
They are a couple folkd in my group that have gained some weight back with the DS like other wls surgeries, there are a couple of folks with the rny as well and they seem pickier about how and what they eat then other folks. Most of the people in group I know don't really have issues with food. I'm lucky I don't sem to have any. A member of my family just had DS done last week can't wait to see the weight come off and got another one in the wings waiting.
If I saw your profile right your in colorado. Your doctor does RNY or Sleeve maybe not DS a sleeve by itself is pretty good I have lost over 300 pounds with it as other folks in my group are getting good results too. IF you need the bypass for comorbidities and you want the DS over RNY and your surgeon doesn't do it look for Gary Anthone here in Omaha NE he is as good as it gets with the DS.
Good luck

Bypass was about 5 grand cheaper than the DS however, I love food and feel I needed something to help me control what I eat, such as the DS only absorbing 30% of what you eat, so u munch all day. This surgery just fit me better.
Im very sore, but can eat full foods on my 1 month anniversary. So it's all good. Some people do have a lot of diarrhea with DS, mostly cause of carbs, flour or sugars if I'm not mistaken. I start my vitamins tomorrow which is only 4 a day. I got the vitamin d shot at my doc office, so another pill I don't need to take. DS vitamins, round about 60/90 bucks a month. And labs are once a yr, some people get more often, and are 600/750 each lab draw. Thank god u have insurance!
Either way u choose, not every surgery is right for everyone, to me it boils down to what eating regimen you can really stick with. Good luck in whatever choice you make, also keep in mind that there are a high number of revisions from bypass to DS due to high failure rate. U really have to eat how ur supposed too. As to DSERS. stick to vites n labs n ur good. ...
Much love, misty
