
Will WLS Resolve All Common Co-Morbid Conditions?
August 20, 2020Will WLS Resolve All Common Co-Morbid Conditions? The shorter answer is yes for the most part.
For co-morbid conditions, there are two variables that need to be clarified before an answer can be given to the question definitively.
The resolution of co-morbidities is a very broad and vague term.
For the purposes of our discussion, I will distinguish between the improvement of co-morbidities and the remission of co-morbidities. This distinction needs to be made since conditions that will significantly improve, however, they will not be completely resolved after weight loss surgery.
They're also conditions where even though they are resolved after weight loss surgery, do you to lack of long-term data, we are inclined to define them to be in “remission”.
Clearly, different weight loss surgical procedures have different success rates.
The success rate may be measured in terms of weight loss, longevity after weight loss in addition to the resolution of co-morbidities. Some of these co-morbid conditions may be directly related to excess weight.
Different weight loss surgical procedures also have different success rate with resolution of co-morbidities.
The review of data collected was reviewed (Sudan et.al (SAORD, 11-2015, S1-S24) has shown that Duodenal Switch was best for weight loss, type II diabetes, and hypertension resolution. Gastric bypass improved GERD. There was no difference for 1-year mortality between DS, GB, and Sleeve.
Co-Morbid Conditions
Diabetes
Type I diabetic patients may benefit from a reduction in the dose of the insulin and improvement of other co-morbidities with weight loss surgery indirectly.
Type II diabetic patients get normalization of HgA1c, as well as reduction and elimination of the diabetic medications. This may include insulin if the patient has been on it for less than 10 years. There appears to be a significant reduction in the rate of remissions in patient with type II diabetes who have been on Insulin for more than 10 years.
Overall, the duodenal switch operation has been the most successful procedure with an over 98% remission rate of type II diabetes for over 10 years post-op. (Kashyap et.al Cleve Clin J Med. 2010 July ; 77(7): 468–476)
Hypertension
Hypertension is seen frequently to improve or completely resolve with weight loss surgery. The efficiency of each procedure for the resolution of HTN is not clearly defined. This is primarily due to the fact that different studies have defined “resolution”, “cure”, and “improvement” on different scales. There is however a general consensus that Duodenal Switch, Gastric Bypass, Sleeve Gastrectomy is the order in which the hypertension is improved or resolved and maintained long term.
(Schiavon et.al, Circulation 2018:137:1132-1142),
(Cohen, et.al, Curr Cardiol Rep. ; 19(10): 98.),
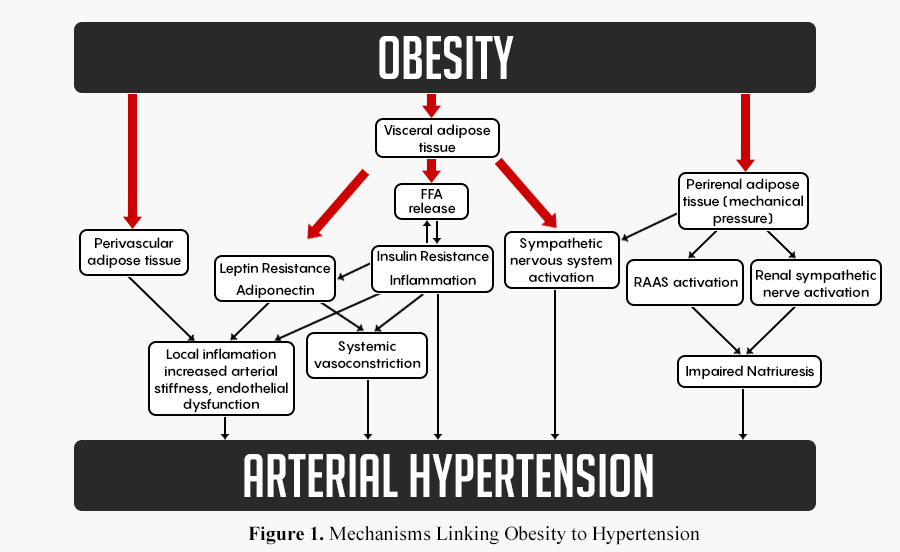
The mechanism of action for obesity is outlined in Figure 1. Fantin et. al. proposed a number of pathways connecting Obesity and Arterial Hypertension. (Fantin et.al, Nutrients 2019, 11, 1667), The different proposed mechanisms may explain the differences between the rate of resolution of hypertension after different weight loss surgical procedures as well as the long term success of each.
It appears that the common denominator for resolution of co-morbidities is the presence or absence of a “metabolic condition”
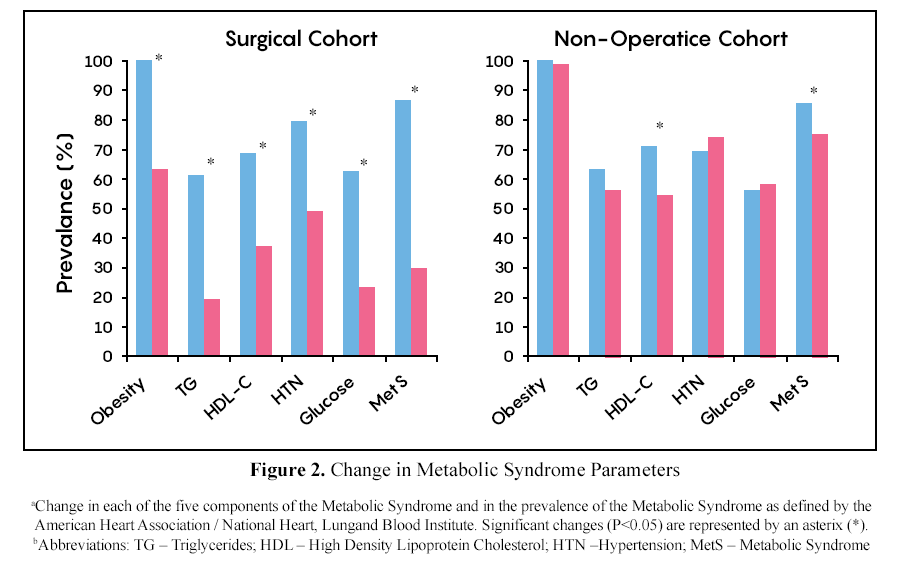
Batsis et. al(Mayo Clin Proc. 2008 August; 83(8): 897–907) (Figure 2 above) demonstrated that the surgical procures improve all the conditions associated with metabolic syndrome. They observed that the resolution of the co-morbidities of metabolic syndrome was related to % excess weight loss.
To be noted is that this study did not look at the Duodenal Switch. However, since the Duodenal Switch operation results in the highest % excess weight loss, AND most sustained % excess weight loss it is not surprising that we see the best result of the resolution of all co-morbid conditions with the Duodenal Switch operation.

Weight Loss: The outcome of DS operation as measured by percent weight loss (Figure 3) has been shown to be superior to the alternatives. (Skogar OBES SURG (2017) 27:2308-2316.)
Reflux
Reflux is seen in both those seeking weight loss surgery and in some cases those who have had with loss surgery.
The cause of the reflux may be 1-Anatomic, or 2-Physiologic.
1-Hiatal hernia, might be causing the reflux. This is a condition where surgical repair is critical to avoid long term damage to the esophagus. Most of the cases are identified before or during surgery when they are repaired.
2-Central obesity, weight gain after panniculectomy, pregnancy, are examples of physiological cause for reflux. These usually are seen with no evidence of a hiatal hernia. In most of cases when the underlying cause is addressed the reflux resolves.
In general, however, any procedure that relies on making the stomach tight as a restrictive measure would be avoided in those patients with reflux.
This is because the procedures will worsen the intragastric pressure, and exacerbate the reflux. Lap-band, Gastric sleeve, and SIPS/SADI should be avoided.
We do routinely, however, do the Duodenal Switch operation on patients with physiologic reflux. This is because we can allow a larger stomach in some cases and accommodate for the larger volume by adjusting the length of the common and alimentary limb to attain the weight loss.
We distinguish ourselves by not doing the length of the small bowel in a cookie-cutter fashion, but rather tailing the length of the common and alimentary length as a percentage of the total length to accommodate for patient metabolic conditions and co-morbidities.
Pseudotumor Cerebri also known as intracranial hypertension causes headaches and in some cases vision disturbances. The underlying cause of this reduced drainage of the CSF caused by central obesity. Weight loss surgery is more effective is mitigating this debilitating headache better than the conventional peritoneal shunt. (Sugerman et.al Annals or surgery, 1999, Vol 229 No 5, 645-642)
Will WLS Resolve All Common Co-Morbid Conditions Summary
The outcome of different weight loss surgical procedures has not been constantly described. Some publications have reported improvement of certain co-morbidities whereas other publications have reported complete remissions.
In some cases, the reports have limited observation for a short period of time (months,3-24) and others have reported long term data (years). The very broad and rather confusing set of information does not lend itself to created distinct clear cut recommendations.

The table above outlines (with references) the published data based on which recommendations are made. Let's remind ourselves that this is not as clear cut and it leaves significant room for a surgeon's experience with peer operative care, and work up.
Based on this information a simple flow chart is proposed. It is important to remember consult your surgeon for the definitive treatment option.


 | ABOUT THE AUTHOR Dr. Ara Keshishian is Director and Surgeon at Central Valley Bariatrics. He has performed more than 2,000 Duodenal Switch procedures and 500+ revisions from other procedures such as RNY, Lap-Band & VSG to the DS since 1999. He has published several research articles on weight loss surgery topics.Read more articles from Dr. Keshishian! |


